

Blood Pressure Medications Explained: What They Do, How They Work, and What to Watch For
Dec 31, 2025
How Blood Pressure Medications Work: Types, Effects & What to Watch
Blood pressure medication can feel confusing, especially when you hear names that sound like chemistry homework: lisinopril, amlodipine, losartan, hydrochlorothiazide.
Here's the good news: most blood pressure medicines fall into a handful of predictable classes. Once you understand the "why," the medication list makes a lot more sense.
I'm going to walk you through the major categories, exactly how they work, common side effects you might experience, and the questions I want you to ask your clinician.
Important medical disclaimer: This is general education only. Do not start, stop, or change blood pressure medication without medical guidance. If you have signs of an allergic reaction, fainting, severe swelling, chest pain, or neurologic symptoms, seek urgent care immediately.
Key Takeaways
Common first-line medication classes include thiazide-type diuretics, ACE inhibitors, ARBs, and calcium channel blockers.
Many people need more than one medication to reach their blood pressure goal.
The "best" medication depends on your other conditions: kidney disease, diabetes, heart disease, pregnancy, or specific side effect concerns.
Why Medication Is Sometimes Necessary (Even With Lifestyle Changes)
Lifestyle is foundational. Exercise, less sodium, more potassium, weight loss, all proven. But medication is often needed because:
Genetics matter enormously. If your parents had high BP, you likely inherited the predisposition.
Arteries stiffen over time due to age and plaque buildup, making it harder for them to relax.
Kidney regulation of sodium and fluid is complex and doesn't always respond to diet alone.
The goal is long-term organ protection: preventing heart attacks, strokes, kidney disease, and heart failure.
Think of medication as "reducing the pressure load" on your heart, brain, kidneys, and blood vessels so they stay healthy for decades.
Infographic Summary:
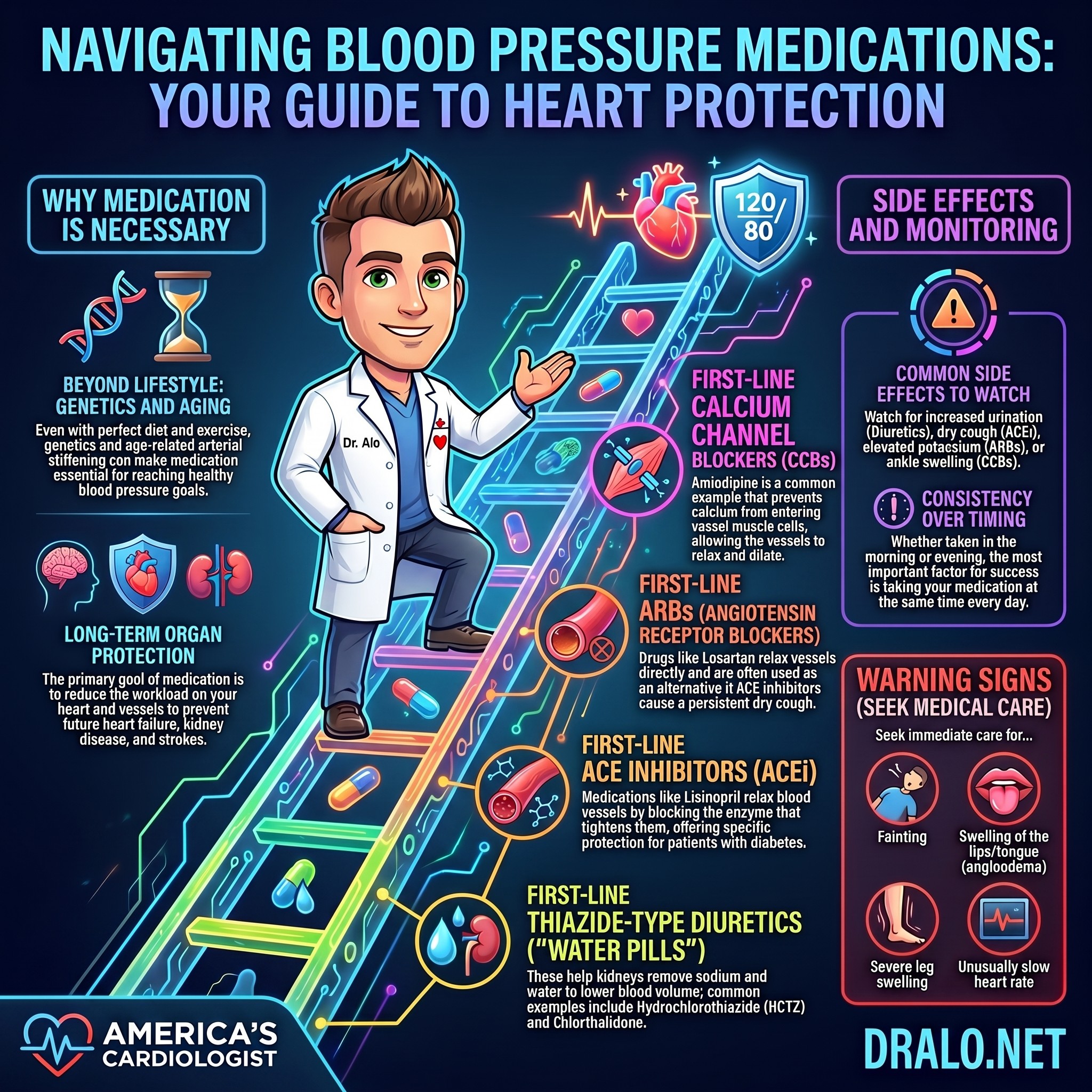
First-Line Blood Pressure Medication Classes (Most Common Starters)
1. Thiazide-Type Diuretics ("Water Pills")
How they work:
Help your kidneys remove sodium and water from your bloodstream
Lower blood volume and vascular resistance over time
Cause vasodilation (blood vessels relax and open up)
Reduce inflammation and endothelial damage because less salt circulating means less irritation
Common examples:
Hydrochlorothiazide (HCTZ)- start here, most commonly prescribed
Chlorthalidone - longer acting, sometimes more potent
Indapamide - alternative with slightly different side effect profile, more vasodilatory effects
Common side effects:
Increased urination (usually early on, often wears off after a few days)
Low potassium or low sodium (your clinician monitors labs)
Possible gout flares in susceptible individuals (diuretics can raise uric acid)
Can slightly worsen insulin resistance if you're prediabetic or diabetic (not an issue if you don't have that genetics)
Important caution: Use with caution in elderly patients due to risk of hyponatremia (low sodium). Your clinician should monitor electrolytes.
2. ACE Inhibitors (ACEi)
How they work:
Block angiotensin-converting enzyme, which normally tightens blood vessels
Result: blood vessels relax by reducing angiotensin II, a potent vasoconstrictor
Can protect the kidneys in certain patients (especially those with diabetes)
Reduce inflammation in blood vessel walls
Common examples:
Lisinopril - start here, very potent and well-tolerated
Enalapril
Benazepril
Ramipril - almost no effect on BP at highest dose
Common side effects:
Dry cough (in some people, happens because ACE inhibitors increase bradykinin, which irritates airways)
Elevated potassium (kidneys hold onto potassium more)
Changes in kidney function (your clinician monitors creatinine and GFR through blood tests)
Dizziness, especially when starting or increasing dose
Rare but serious swelling reaction called angioedema (swelling of lips, tongue, or throat—seek emergency care if this happens)
Why we often start with these: They're very potent, well-tolerated, and provide kidney protection in diabetes and chronic kidney disease.
3. ARBs (Angiotensin Receptor Blockers)
How they work:
Block the angiotensin II receptor directly (similar pathway to ACE inhibitors, but different mechanism)
Result: blood vessels relax
Often work without the cough that some people experience on ACE inhibitors
Common examples:
Losartan — start here, most available and best tolerated
Valsartan
Candesartan
Irbesartan
Common side effects:
Elevated potassium (similar to ACE inhibitors)
Changes in kidney function (labs monitored)
Dizziness, especially when starting
Dry cough is very rare with ARBs (unlike ACE inhibitors)
Key point: If you get a cough on an ACE inhibitor, switching to an ARB often resolves it while maintaining the same blood pressure-lowering effect.
4. Calcium Channel Blockers (CCBs)
There are two main types, and they work very differently:
Dihydropyridine CCBs (Commonly Used for Blood Pressure)
How they work:
Block calcium from entering smooth muscle cells in blood vessel walls
Result: blood vessels relax and dilate
Also reduce peripheral vascular resistance
Common examples:
Amlodipine - most commonly prescribed, long-acting, excellent tolerability
Nifedipine (extended release) - immediate release forms can cause reflex tachycardia, so extended release preferred
Felodipine
Common side effects:
Ankle swelling (peripheral edema due to vasodilation)
Flushing (facial redness and warmth)
Headache (from vasodilation)
Constipation (more common with certain CCBs like diltiazem)
Note on ankle swelling: This is different from heart failure swelling. It's from the medication dilating blood vessels, not a sign of fluid overload. Talk to your clinician if it's bothersome; dose adjustment sometimes helps.
Non-Dihydropyridine CCBs (Different Purpose, Not Ideal for BP Alone)
Examples: Diltiazem, verapamil
Why we distinguish: These slow the heart rate more and are used for specific reasons (certain arrhythmias, angina), not as first-line BP treatment.
Why Many People Need Combination Therapy
Blood pressure is regulated by multiple systems: blood volume, blood vessel tone, hormones (angiotensin, aldosterone, sympathetic nervous system).
One medication often isn't enough to reach goal BP.
For stage 2 hypertension, guidelines often recommend starting with two first-line agents from different classes, ideally in a single-pill combination to:
Simplify the regimen (one pill instead of two)
Improve adherence (people take meds more consistently)
Reach BP goal faster
Examples of dual-therapy combinations: ACEi + diuretic, ARB + calcium channel blocker, diuretic + calcium channel blocker.
Other Blood Pressure Medication Classes (Used for Specific Scenarios)
Beta Blockers
How they work:
Slow heart rate and reduce cardiac output
Reduce effects of sympathetic nervous system (fight-or-flight)
Key point: Beta blockers are generally NOT first-line for uncomplicated hypertension, but they're essential when you have conditions like:
Coronary artery disease or prior heart attack
Heart failure with reduced ejection fraction
Certain arrhythmias
Common side effects:
Fatigue (very common, especially early on)
Lower exercise tolerance in the beginning
Low heart rate
Erectile dysfunction (in some men)
Can slightly worsen insulin resistance if you're prediabetic or diabetic (not an issue without those genetics)
Why we avoid them in young people: Fatigue, reduced exercise capacity, and sexual dysfunction are poorly tolerated and alternatives often work better.
Mineralocorticoid Receptor Antagonists (MRAs)
Example: Spironolactone
How they work:
Block aldosterone, a hormone that causes sodium and water retention
Often used in resistant hypertension (BP not controlled on three agents) or heart failure
Potential issues:
High potassium (serious concern—kidney function and other medications matter)
Breast tenderness in some patients (spironolactone specifically)
When used: Usually not first-line, reserved for resistant hypertension or specific heart conditions.
Alpha Blockers and Central Alpha Agonists
Examples: Prazosin, doxazosin, clonidine, methyldopa
These can be useful, but they're typically not first-choice for routine hypertension. They require careful monitoring for dizziness and other side effects.
When to Take Your Blood Pressure Medication (And Why It Matters)
This is one of the most common questions I get, and the answer is: it depends on the medication and your individual situation.
Morning vs. Evening: The Evidence
Morning dosing: Traditionally recommended because BP is naturally higher in the morning (morning surge).
Evening dosing: Some evidence suggests evening dosing may be slightly better for 24-hour BP control and may reduce cardiovascular events slightly more.
Bottom line: Consistency matters more than timing. Take your medication at the same time every day. If you miss a dose, take it as soon as you remember (unless it's close to the next dose, then skip the missed dose).
Ask your clinician: "Should I take my blood pressure medication in the morning or evening, and why?"
Important Questions to Ask Your Clinician
What is my BP goal based on my overall risk profile? (Goal varies: lower risk = 130-139; higher risk = under 130)
Which medication class is best for my other conditions? (Kidney disease? Diabetes? Heart disease? Pregnancy? Each changes the answer.)
What side effects should I watch for, and what should I ignore? (Some side effects go away; others signal you need a change.)
Do I need lab monitoring, and how often? (Kidney function, potassium, sodium—depends on your medications and baseline kidney health.)
When should I take it and why? (Morning vs. evening, with or without food.)
What should I do if I miss a dose? (Take as soon as remembered, or skip to next dose? Depends on the medication.)
How will we measure success? (Home BP averages? Office readings? Both? This matters because of white coat and masked hypertension.)
What combinations of medications work best together? (Some combinations are more effective than others.)
Why Medications "Don't Work" (Usually It's Not the Drug)
The most common reason blood pressure meds appear ineffective is NOT that they're inherently ineffective, but rather:
BP is being measured incorrectly. Wrong cuff size, talking during measurement, not resting—all skew readings high.
Doses are missed because the regimen is too complicated (three different pills at different times).
Side effects weren't addressed early. You get a headache or dizziness, assume the drug doesn't work, and stop it without telling your clinician that a dose adjustment might fix it.
Home and office BP numbers don't match. You have white coat hypertension (high in office, normal at home) or masked hypertension (normal in office, high at home), so you and your clinician are looking at different data.
The fix: Team-based care, good home BP data, and honest communication about side effects.
How Long Does It Take for Blood Pressure Medication to Work?
This is one of the most frequently asked questions.
The answer: It depends on the medication and your body.
Most medications lower BP within hours to days of starting. However, it can take 2-4 weeks at a given dose to see the full effect.
Some medications have a longer onset: losartan and lisinopril take 1-2 weeks; amlodipine takes 6-8 days.
Important: Don't judge a medication's effectiveness in the first week. Give it time. And don't stop it because you feel "fine"—that often means it's working.
Can I Combine Blood Pressure Medication With Supplements?
This is critical because people often ask me about magnesium, CoQ10, beet juice, and other supplements while on BP meds.
Magnesium + Blood Pressure Medication
Generally safe, but magnesium can enhance the effect of calcium channel blockers. Talk to your clinician before starting magnesium supplements, especially in high doses.
Beet Juice + Blood Pressure Medication
Likely safe, but beet juice contains nitrates that can lower BP. The combination isn't dangerous, but your clinician should know. BP might drop a bit more than expected.
Viagra/Erectile Dysfunction Medication + Blood Pressure Medication
This combination needs caution, especially with nitrates or certain BP meds. Never combine Viagra with nitrates (nitroglycerin). Talk to your cardiologist before taking ED medication if you're on blood pressure meds.
Warning Signs: When to Call Your Clinician
Fainting or severe dizziness (especially upon standing)
Swelling of lips, face, or tongue (possible allergic reaction or angioedema)
Severe leg swelling or new shortness of breath
Unusually slow heart rate (under 50 bpm)
Muscle weakness, cramping, or severe fatigue (possible electrolyte issues)
Persistent cough (may need to switch medications)
Severe headache or blurred vision
Don't ignore these. Call your clinician or seek urgent care.
The Bottom Line
Blood pressure medication is a powerful tool for preventing heart disease, stroke, and kidney failure. Understanding your medication—what it does, why you're on it, what to watch for—makes you a better partner in your own care. Ask questions. Take your medication consistently. Monitor your BP at home. And tell your clinician about side effects early so they can adjust your plan if needed.
Ready for personalized guidance on your blood pressure medications? Join the Heart 2 Heart VIP Community where you can text me medication questions any time, join live video calls to discuss your BP management plan, and connect with others navigating hypertension treatment. No generic answers—just evidence-based cardiology.
💪🏻🩺🫀 Dr. Alo
References:
Related Blood Pressure Management Posts
- What Does 130/80 Mean?
- How to Take BP at Home
- Why BP High Morning?
- White Coat vs Masked
- BP Spikes
- When BP Emergency?
- Low BP Symptoms
- Foods Lower BP
- Lower BP Naturally
- Salt & Heart
- Dietary Guidelines
- Statins & Dementia
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















