

Is Diabetes Genetic? What Can You Do About It?
Sep 30, 2024
Is Type 2 Diabetes Genetic Disorder?
Yes. Type 2 diabetes is absolutely genetic. There is no argument amongst the medical community. But there is a ton of nuance. People don't ever want the nuance. They just want to fall into one of two camps; either it is or it isn't genetic.
While type 2 diabetes is a genetic disorder, that does not mean there is nothing we can do about it. That also does not mean that we just medicate people and not help them with diet, exercise, weight loss, and other lifestyle modifications. I have written entire books on weight loss and give thousands of lectures every year on how to lose weight properly. They are all available for free on YouTube. I am also an obesity physician and have helped hundreds of thousands of patients lose weight over the years.
This also means that you can weigh 500 pounds and not be diabetic, nor insulin resistant. We have plenty of morbidly obese patients that are not even a tiny bit insulin resistant. If they had even a small amount of insulin resistance, we could get them approved for the newer weight loss medications like Ozempic and Mounjaro. We try every which way to test them for insulin resistance, and they don't have it and can't get the medications.
This does not mean that there is nothing you can do about it.
If you have the genes for diabetes, and gain weight, regardless of what macronutrients you emphasize, you will become more diabetic. The macronutrients emphasized don't matter much. You can gain weight eating high carbs or low carbs, you will still become more insulin resistant and more diabetic.
If you do not have the genes for insulin resistance, you can not become diabetic, even if you gain weight. Even if you eat only sugar. Sugar consumption does not independently make you diabetic.
If you do not have the genes for diabetes, you can eat all the sugar you want, and you will not become diabetic.
Of course, I am not suggesting you should eat sugar, but there are always some people online that want to accuse me of saying people should just eat tons of sugar. You can be diabetic eating only fat. You can be diabetic eating only protein.
Infographic Summary:
Diabetes Genetics
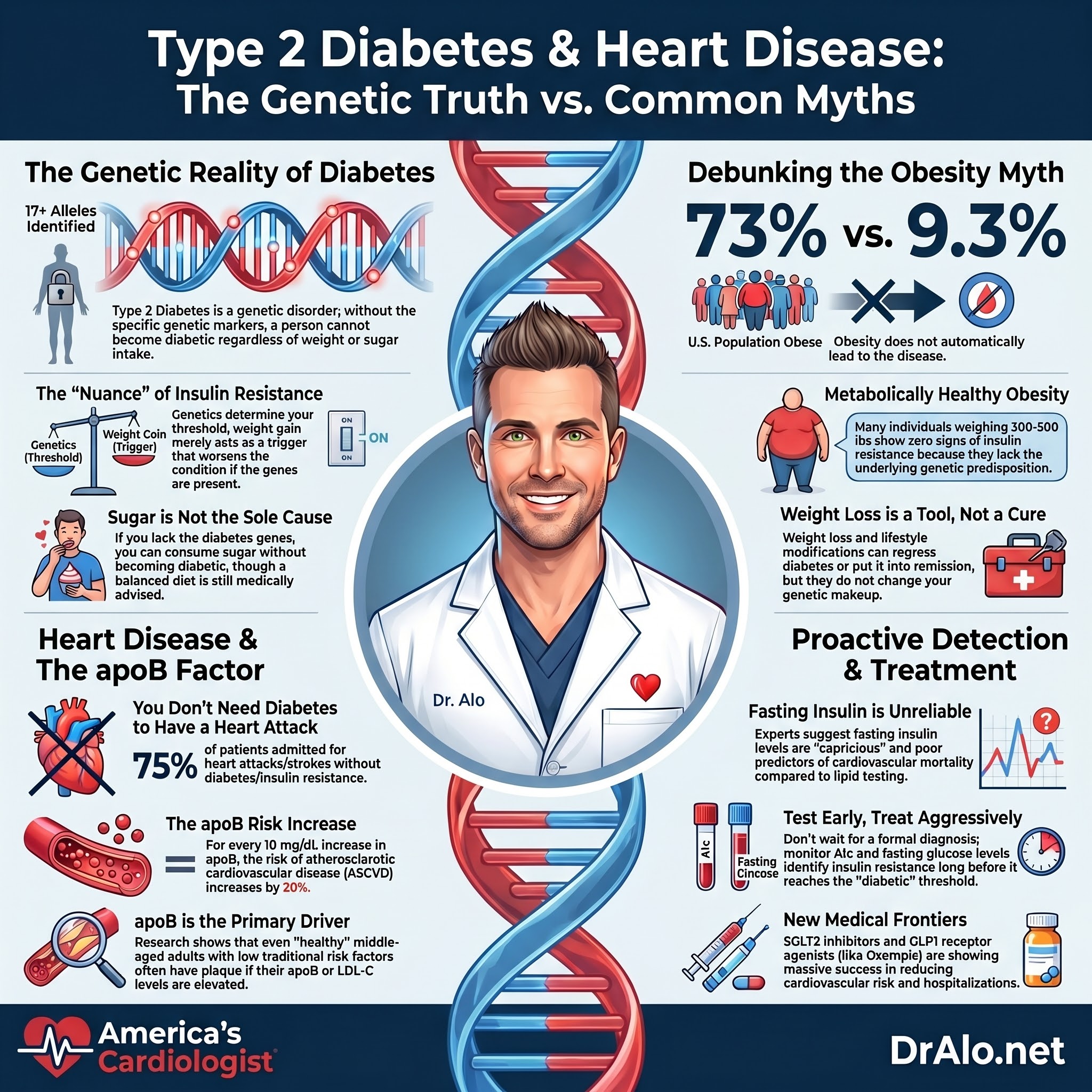
To date, we have identified at least 17 alleles that are responsible for type 2 diabetes genes. Other studies have shown over 77 alleles that code for type 2 diabetes.

The article is a fantastic overview of the genetics of diabetes and all the progress we have made in this field:
https://pubmed.ncbi.nlm.nih.gov/18782870/
Other studies on the genetics of type 2 diabetes:
https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.119.316065
https://diabetesjournals.org/care/article/45/3/674/141024/Type-2-Diabetes-Partitioned-Polygenic-Scores
It's Not Just About Sugar: The Surprising Genetic Roots of Type 2 Diabetes
Most people think of type 2 diabetes as a "lifestyle disease": eat too much, move too little, and eventually blood sugar goes haywire. But decades of research tell a much more nuanced story. Genetics plays a massive role, and the science behind it is genuinely fascinating.
Your Family Tree Matters, A Lot
One of the most compelling lines of evidence comes from good old-fashioned family studies. Having just one parent with type 2 diabetes gives a person roughly a 40% lifetime risk of developing the disease. If both parents are affected, that number climbs to nearly 60–70%. Full siblings of someone with type 2 diabetes face a 30–60% increased risk compared to the general population. That kind of clustering in families goes well beyond shared eating habits.
Twin Studies: Nature's Experiment
Twin studies are the gold standard for teasing apart genes from environment. Identical (monozygotic) twins share 100% of their DNA, while fraternal (dizygotic) twins share about 50%. If a disease were purely environmental, concordance rates should be similar in both groups. But for type 2 diabetes, concordance in identical twins ranges from 60–90%, compared to only 20–30% in fraternal twins. When impaired glucose tolerance is included, concordance in identical twins jumps to as high as 88%. Overall heritability estimates for type 2 diabetes land in the range of 30–72%, depending on the population studied.
A landmark Danish twin study confirmed this multifactorial picture: heritability for abnormal glucose tolerance was estimated at 61%, supporting the idea that genetic predisposition is critical for developing glucose intolerance, even if environmental factors determine whether someone tips over into full-blown diabetes.
The Genome-Wide Revolution: Over 700 Risk Variants and Counting
The real explosion in understanding came with genome-wide association studies (GWAS). These massive studies scan the entire genome across hundreds of thousands of people to find DNA variants linked to disease. The results have been staggering: researchers have now identified more than 700 genetic loci associated with type 2 diabetes risk. The largest multi-ancestry GWAS to date, the DIAMANTE Consortium, analyzed over 180,000 people with type 2 diabetes and 1.1 million controls across diverse populations, identifying 237 loci at stringent genome-wide significance.
These genetic variants collectively explain close to 50% of type 2 diabetes heritability. Most individual variants have only a small effect on risk, but together they paint a picture of a disease deeply embedded in our DNA.
The Star Player: TCF7L2
Among all the genetic variants discovered, one gene stands out: TCF7L2. It is the strongest common susceptibility locus for type 2 diabetes, associated with impaired beta-cell function and carrying an odds ratio of about 1.4 per risk allele. Other notable genes affect insulin secretion (KCNJ11, SLC30A8, CDKAL1), insulin sensitivity (PPARG, IRS1), or both pathways.
Genetics Hit Harder in Young People
An intriguing finding is that genetics appears to contribute even more to early-onset type 2 diabetes than to adult-onset disease. The first GWAS in young people with type 2 diabetes found that both common and rare genetic variants contributed 3–5 times more to disease liability in youth compared to adults. This suggests that when type 2 diabetes strikes early, it is often on a particularly strong genetic background.
Genes + Environment = The Full Picture
None of this means lifestyle doesn't matter; it absolutely does. The current understanding is that type 2 diabetes develops on a predisposing genetic background, with obesity and sedentary behavior acting as triggers in genetically susceptible individuals. A prospective study from the Malmö Preventive Project illustrated this interaction beautifully: individuals with the highest genetic burden (12 or more risk alleles) in the highest BMI quartile had an eightfold increased risk of developing diabetes.
Figure 2 Nongenetic and Genetic Risk Factors for Type 2 Diabetes in the Malmö Study. undefined
Can You Reverse Diabetes?
It's nuanced.
While you can not change your genes, you may be able to regress your diabetes or put it into remission. Some people have a mild case of insulin resistance, and can regress that insulin resistance with weight loss. This will work regardless of how you lose the weight and regardless of which macronutrients you emphasize.
Some people have worse insulin resistance and will not be able to get off meds or reverse their diabetes as much.
Some people with severe diabetes can be super thin and still have diabetes. They will just need medications. They can also attempt to build muscle, which will help.
Why Do I Care So Much About Diabetes?
Before I became a cardiologist, I was an internist. Internal medicine physicians are very well trained in diabetes management. Cardiologists can be as well, but most usually defer diabetes management to primary physicians and or endocrinologists.
During my internal medicine training, I rotated with an endocrinologist many times because I was so fascinated by diabetes and insulin resistance. He was based out of Chicago and had been involved in many diabetes trials over his 30-year career. To this day, I call him, and we discuss the latest and greatest in diabetes care and treatment. I loved endocrinology so much that I did extra rotations in endocrinology.
I am in rural Ohio. Many times, I am the only physician the patient will see. Most rural regions have non-physicians as their primary care providers. I am more well trained in managing diabetes than most non-physicians.
It’s important for cardiologists to master diabetes care. Especially with the new SGLT2 inhibitor medications like Invokana, Jardiance, and Farxiga and the new GLP1 receptor agonists like Ozempic and Mounjaro (and others) that have shown tremendous cardiovascular risk reductions, improved outcomes, and less hospitalizations. These medications are going to be incorporated into most cardiovascular guidelines. The SGLT2 inhibitors are already indicated and in the guidelines for many cardiac conditions, and the GLP1 RAs will be next. If you are a healthcare provider that wants to get started in Obesity Medicine, grab my masterclass.
My biggest pet peeve in all of medicine is that we wait 10-15 years before we tell a patient that they are diabetic. We wait until their fasting glucose is over 125 mg/dL and their A1c is over 6.5%. This is the official diagnostic criteria and that’s generally why most clinicians wait.
The concern is that most patients are insulin resistant long before they cross the threshold of fasting blood glucose over 125 mg/dL and A1c of 6.5%. We need to treat it earlier and be more aggressive.
Diabetes is the leading cause of blindness, renal failure, amputations, and neuropathy in the world. I am very passionate about diabetes care, early detection, and treatment.
We know when someone is insulin resistant long before they are officially “pre-diabetic”. Pre-diabetes is defined by having a fasting glucose level of 100 mg/dL or higher, but not yet above 125 mg/dL.
So how can you diagnose pre-diabetes or diabetes earlier? It’s not that hard. Just look at their A1c or fasting glucose. You can even do an oral glucose tolerance test if you want more data.
You Don’t Need Insulin Resistance To Have Heart Disease
Another myth circulating is that the only way to end up with ASCVD is to have insulin resistance. This is probably the easiest myth to dismiss. As you may have noticed in the previous chapter or blog posts, insulin resistance was not present in those who developed ASCVD.
Starting from the simplest explanation, teenagers with familial hypercholesterolemia do not have insulin resistance. They are lean, healthy, active, eat well-balanced, healthy diets, and many of them are athletes.
Secondly, the incidence of type 2 diabetes in the US and worldwide is about 9.3% of the population. This is not a very high number.
But let’s look at the data.
Researchers set out to answer this exact question. They evaluated children with familial hypercholesterolemia. These are kids with genetically incredibly high cholesterol. They have LDL-C over 190 mg/dL. One in about 200 to 300 people have this form of elevated cholesterol. It’s called FH (familial hypercholesterolemia). See the posts on that for more.
In a 2018 study, they included children ages 4-18 who had FH. They used fancy testing to test for insulin resistance long before it actually manifests. They used HOMA-IR (Homeostatic Model Assessment) by performing oral glucose tolerance test (OGTT). The BMI of these young participants was 20 kg/m2 (not overweight). Their conclusion was, “No relationship was identified between lipid profiles and insulin resistance”.
However, they did find that the participants that had insulin resistance had higher concentrations of apoB. Which is why we harp on apoB measurement so much. Because that is the causative agent. We know that insulin resistance can increase plasma residence time of lipoproteins, which is why apoB (LDL-C) is elevated.
You can read the study at:
https://www.degruyter.com/document/doi/10.1515/jpem-2018-0337/html
You may argue that that was a small study, the sample size was low, or that in the end they still concluded that people with FH had slightly more insulin resistance than not. Understood. What if we looked at a huge population, not just 77 kids?
Another study looked at 63,000 individuals with FH and found that the prevalence of diabetes was only 1.75%. So, despite having a much lower incidence of IR, these FH patients still had high levels of ASCVD. They actually had less insulin resistance than the general population.
https://jamanetwork.com/journals/jama/fullarticle/2190985
Another study found that having FH actually protected people from developing diabetes. So, despite low IR, they still had very high levels of ASCVD.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9002616/
One important point, patients with FH have larger, more buoyant, LDL particles (often erroneously and sophomorically referred to as “large and fluffy”) and have the worst form of atherosclerosis with the shortest lifespans. See my other blog posts on particle size and density.
How can it be insulin resistance when only about 9% of the world’s population has diabetes, yet most people have heart disease and die of heart disease? The cholesterol disputers have no answer to this.
In case you are questioning these numbers, the global prevalence of diabetes in 2019 was 9.3% of the population, or about 463 million people worldwide. It is expected to rise to 578 million by 2030, which is 10.2% of the population. In another report, based on CDC data, the prevalence of diabetes was a bit higher at 11.6%.
https://pubmed.ncbi.nlm.nih.gov/31518657/
https://www.cdc.gov/diabetes/data/statistics-report/index.html
Does Obesity Cause Diabetes?
One point that is important to point out at this juncture is that obesity does not cause diabetes. Diabetes is a genetic disorder that can be worsened by obesity. We have gone over the genetics of diabetes earlier. You cannot give yourself diabetes by overconsuming calories and becoming obese. That’s not how it works.
Think about it in simple logical terms. We know that 73% of the US population is obese. Yet only 9.3% (depending on the study) have diabetes. There are plenty of overweight patients that weigh over 300 or 400 pounds that have A1c levels that make most people jealous.
This means that a majority of obese individuals are “metabolically healthy” with insulin sensitivity similar to normal weight individuals.
The prevalence of metabolic syndrome in the US is around 15-31% of the population (depending on study) and this does impart a twofold increase in cardiovascular disease. Without question. That’s not the issue here. But 31% is not 73%. Not all overweight and obese individuals end up with diabetes.
In the US, about 40% of the population is considered obese and only 30% of obese patients have metabolic syndrome in case you were curious.
https://link.springer.com/chapter/10.1007/978-3-319-48382-5_1
https://www.cdc.gov/nchs/fastats/obesity-overweight.htm
What about people that have very high insulin levels due to insulinomas? These are insulin secreting tumors. These individuals have very high levels of insulin, with no evidence of increased atherosclerosis. You could argue that having insulin secreting tumors is not the same thing as having high insulin levels due to insulin resistance. True, but both result in very high insulin levels.
Here are those studies:
https://pubmed.ncbi.nlm.nih.gov/23908245/
https://pubmed.ncbi.nlm.nih.gov/21430026
https://pubmed.ncbi.nlm.nih.gov/8144864/
The final nail in the coffin? Only 25-30% of patients admitted to the hospital with acute coronary syndrome (heart attacks), actually had diagnosed diabetes. So, 75% of heart attack and stroke patients do not have diabetes nor insulin resistance at all.
Study:
https://pubmed.ncbi.nlm.nih.gov/35245735/
Again, this all points to the conclusion that you need to have the underlying elevated LDL-C first. If you have elevated apoB, then everything else falls into place. Without apoB, there is no ASCVD.
Young And Full Of Disease
In July of 2024 an article was published in the Journal of the American College of Cardiology that wanted to answer this exact question. Can young people without any of the traditional risk factors still get heart disease? And what causes it?
They looked at adults aged 40 to 65 that had a 10 year risk score of less than 5%, meaning their risk for ASCVD is very low when looking at the traditional risk factors, age, weight, BMI, diabetes, smoking, kidney function, metabolic parameters, and other metrics. By all objective measures, these were people with a very low risk of heart disease.
They even looked at the presence of calcium or soft plaque in the heart.
They found that most had plaque and it was worse and more prevalent the higher the LDL-C or apoB. The graphics from this paper are quite impressive and I highly recommend you take a look in the supplemental guide.
They also found that for every 10 mg/dL increase in LDL-C or apoB, you had a 13% and 20% increase in ASCVD, respectively. As an example, nearly 70% of men with an apoB over 120 mg/dL had ASCVD. The number was 60% for LDL-C over 160 mg/dL.
They concluded,
“Among healthy asymptomatic middle-aged adults without traditional ASCVD risk factors in the U.S., coronary atherosclerosis on CCTA is common even at lower serum levels of LDL-C, non-HDL-C, and apoB. Coronary atherosclerosis is more prevalent at higher levels of serum lipoproteins for both men and women, and high-risk plaque features are present but relatively infrequent in low-risk adults. These findings emphasize the importance of lipid-lowering strategies to prevent the development and progression of atherosclerosis in adults regardless of risk factors”.
Study:
https://www.jacc.org/doi/10.1016/j.jacadv.2024.101049
Fasting Insulin and Insulin Resistance Are Not Reliable
Another issue that comes up frequently among the Medfluencer crowd is that cholesterol doesn’t matter if you don’t have insulin resistance. Or they will claim that the “root cause” of all cholesterol problems is insulin resistance and not actually LDL-C. If you have made it this far, you know this is nonsense at this point.
They say that a fasting insulin level is the best way to determine if insulin resistance is present. The only problem is that fasting insulin has been unreliable over the years and has not been recommended by endocrinologists nor the American Diabetes Association to be useful in predicting insulin resistance.
The gold standard test of insulin resistance in people who are euglycemic (normal blood sugars and not known to have insulin resistance) is a test called a clamp study.
Don’t listen to me here is what the experts have said,
“Prospective mortality studies have shown insulin measures do not predict cardiovascular mortality when metabolic syndrome characteristics, such as lipids, are taken into account. Furthermore, the relationship between clamp insulin resistance and fasting serum insulin level is weak: fasting serum insulin level explains only 36% of variance in insulin resistance, even less when glucose metabolism is impaired. Measurement of serum insulin levels has been described as “fraught with errors and inconsistencies”; a clinician who ordered this inappropriate test would be overwhelmed by poor 120-minute reproducibility, among other problems. By analogy, fasting serum insulin level is a capricious little beast subject to intra-individual variation on any couple of days, and substantial inter-assay and inter-laboratory variations; interpreting fasting serum insulin levels may be considered like wrestling a column of smoke”.
You can read the article at:
https://www.mja.com.au/journal/2006/185/3/insulin-levels-insulin-resistance-phantom-metabolic-opera
Another very well-done study concluded that,
“Fasting insulin sensitivity indices are modest predictors of insulin sensitivity measured by euglycemic clamp, and do not perform better than clinical surrogates in this population”.
You can read that study:
https://bmcendocrdisord.biomedcentral.com/articles/10.1186/1472-6823-14-65
The longest and most well written article on how you should test for diabetes or insulin resistance was just published the American Diabetes Association in July of 2023 and can be found at:
From that link, you can download the 49-page PDF and I highly encourage you to read it.
Diabetes Bottom Line
Type 2 diabetes is not simply a consequence of poor choices. It is a complex, polygenic disease with heritability rivaling that of many conditions traditionally thought of as "genetic." The interplay between hundreds of genetic variants and environmental exposures determines who ultimately develops the disease, and understanding that interplay is opening the door to precision medicine approaches that could transform how type 2 diabetes is prevented and managed.
More References
- Type 2 Diabetes: Principles of Pathogenesis and Therapy. Stumvoll M, Goldstein BJ, van Haeften TW. Lancet (London, England). 2005 Apr 9-15;365(9467):1333-46. doi:10.1016/S0140-6736(05)61032-X.
- Genetic predisposition in type 2 diabetes: A promising approach toward a personalized management of diabetes. Sirdah MM, Reading NS. Clinical Genetics. 2020;98(6):525-547. doi:10.1111/cge.13772.
- The Architecture of Risk for Type 2 Diabetes: Understanding Asia in the Context of Global Findings. Abdullah N, Attia J, Oldmeadow C, Scott RJ, Holliday EG. International Journal of Endocrinology. 2014;2014:593982. doi:10.1155/2014/593982.
- Dissection of Type 2 Diabetes: A Genetic Perspective. Bonnefond A, Florez JC, Loos RJF, Froguel P. The Lancet. Diabetes & Endocrinology. 2025;13(2):149-164. doi:10.1016/S2213-8587(24)00339-5.
- Heritability of Type II (Non-Insulin-Dependent) Diabetes Mellitus and Abnormal Glucose Tolerance--a Population-Based Twin Study. Poulsen P, Kyvik KO, Vaag A, Beck-Nielsen H. Diabetologia. 1999;42(2):139-45. doi:10.1007/s001250051131.
- Current Insights and Emerging Trends in Early-Onset Type 2 Diabetes. Misra S, Ke C, Srinivasan S, et al. The Lancet. Diabetes & Endocrinology. 2023;11(10):768-782. doi:10.1016/S2213-8587(23)00225-5.
- Genetics of Type 2 Diabetes: Implications From Large-Scale Studies. DeForest N, Majithia AR. Current Diabetes Reports. 2022;22(5):227-235. doi:10.1007/s11892-022-01462-3.
- Multi-Ancestry Genetic Study of Type 2 Diabetes Highlights the Power of Diverse Populations for Discovery and Translation. Mahajan A, Spracklen CN, Zhang W, et al. Nature Genetics. 2022;54(5):560-572. doi:10.1038/s41588-022-01058-3.
- Type 2 Diabetes Across Generations: From Pathophysiology to Prevention and Management. Nolan CJ, Damm P, Prentki M. Lancet (London, England). 2011;378(9786):169-81. doi:10.1016/S0140-6736(11)60614-4.
- Clinical Risk Factors, DNA Variants, and the Development of Type 2 Diabetes. Lyssenko V, Jonsson A, Almgren P, et al. The New England Journal of Medicine. 2008;359(21):2220-32. doi:10.1056/NEJMoa0801869.
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















