

Do Statins Cause Diabetes?
Jan 26, 2025
Do Statins Cause Diabetes?
It’s complicated. It depends on what you mean by “causes diabetes”. There’s a lot of nuance. Please read the entire article.
If you already have pre-existing insulin resistance, pre-diabetes, and or diabetes, you are at a slightly increased risk of developing, or worsening your insulin resistance or disease state. Let's take a look.
Studies On Statins And Diabetes Risk
While studies have shown a very mild or moderate worsening of insulin resistance metrics, the fears need to be addressed in a way that addresses the risk of not treating elevated apoB in that population.
Diabetics are at a significantly increased risk of heart disease and need more aggressive lipid lowering therapy. The benefits generally outweigh the risks.
With that said, there is a lot of fearmongering about diabetes with Medfluencers and mainstream media trying to scare people from taking statins because they may end up with diabetes. Which is not possible, unless you already have the genes for diabetes.
Infographic Summary:
Atorvastatin vs Rosuvastatin And Diabetes Risk
A recently published trial comparing long term efficacy and safety of rosuvastatin versus atorvastatin in adults with coronary artery disease demonstrated that the rosuvastatin group had a higher incidence of new onset diabetes requiring initiation of anti-diabetes medications. The absolute difference between rosuvastatin and atorvastatin was 1.8% (9.5% vs 7.7%).
Read the study at:
https://www.bmj.com/content/383/bmj-2023-075837
Studies On Statins And Insulin Resistance
Prior studies have shown a minimal trend towards worsening insulin resistance.
In the JUPITER trial, they took people who had “normal” LDL cholesterols, but high CRP (high inflammation) and placed them on statin therapy. This was a study to see how much of a difference the statin made in people who had no prior heart disease, normal cholesterol, but elevated inflammatory markers. It was a primary prevention trial.
The trial had to be stopped early because it was unethical to continue the placebo arm.
The statin group demonstrated a reduction in every endpoint; myocardial infarction, stroke, revascularization (needing to have a stent placed, or replaced), and death from any cause (all-cause mortality).
https://www.ahajournals.org/doi/full/10.1161/CIRCOUTCOMES.109.868299
Every single subgroup benefited from the statin, see charts in the supplemental guide or click on the study.
What About Diabetes and A1c in the JUPITER Study?
But what about diabetes?
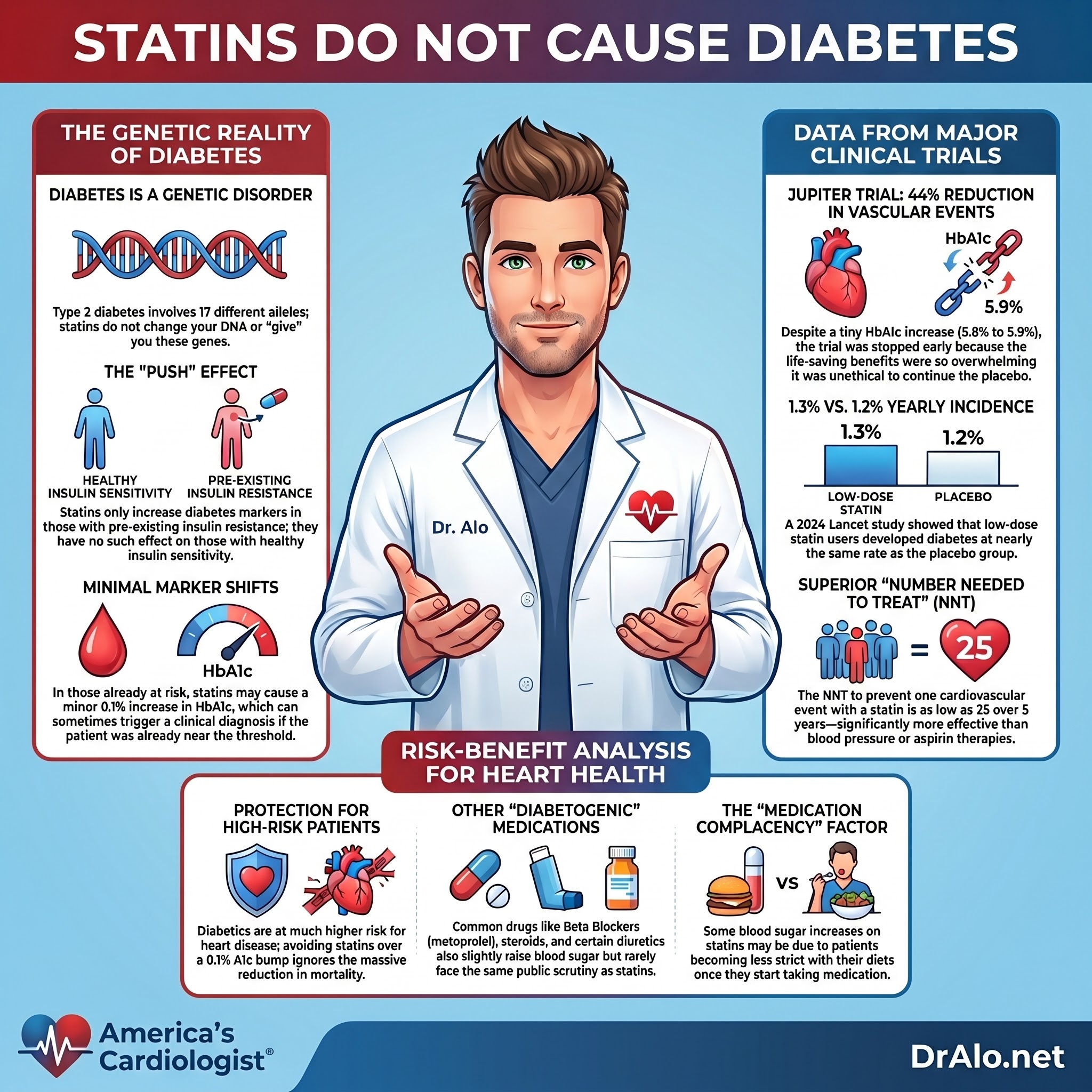
You had an increase in HbA1c from 5.8% to 5.9% in the statin group. If you understand diabetes or have diabetes, you will understand that this is minimal.
The JUPITER trial showed a 44% reduction in all vascular endpoints, and it was the first trial to show a clear benefit in women with a 46% reduction in all vascular endpoints.
What about the number needed to treat? The NNT usually tells us how many people you need to treat with X to prevent one Y. For example, how many people need to be on a statin to prevent one stroke?
Here are the NNT values from the JUPITER trial, I’ll let you read them, they are pretty impressive and among the lowest.
The NNT to prevent one clinical event is a metric of treatment benefit that encompasses both absolute and relative risk reductions and is commonly used to compare treatment strategies. When evaluating NNT values, care must be taken to specify the population under study, as well as the end points and time-frames of interest. Within JUPITER, which enrolled healthy men more than 50 years of age and women more than 60 years of age, the 2-, 3-, 4-, and 5-year NNT values are 95, 49, 31, and 25, respectively for the primary trial end point, and 98, 59, 39, and 32, respectively for the restricted “hard” end point of myocardial infarction, stroke, or death (P.M.R., unpublished data, 2009). All of these NNT values compare favorably to several other therapies widely considered to be effective in the primary prevention of cardiovascular disease. For example, comparable 5-year NNT values for the treatment of hyperlipidemic men such as those enrolled in AFCAPS/TexCAPS and WOSCOPS range between 44 and 63, suggesting that the strategy of screening for elevated hsCRP is at least as effective as the strategy of screening for elevated LDLC.
Perhaps more striking is a comparison to the treatment of hypertension where comparable 5-year NNT values between 86 and 140 have been reported as being cost-effective, or the use of prophylactic aspirin where 5-year NNT values in primary prevention exceed 300 (See figure below). Thus, despite explicitly excluding patients with LDLC >130 mg/dL and including large numbers of women (who have lower event rates than do men), the absolute risk reductions observed in JUPITER and the concomitant NNT values are, if anything, superior to that of statin therapy in the primary prevention of vascular events among hyperlipidemic men or the prophylactic use of antihypertensive or antithrombotic therapies among middle-aged and older men and women.
The JUPITER trial had the lowest 5-year NNT to prevent one cardiovascular event of all comparable trials.
That’s pretty impressive.
Study Published in Circulation on Atorvastatin and Diabetes
A recent article published in Circulation showed that people on atorvastatin 40mg for 10 weeks had a 7-9% increase in most diabetes related markers. This would include people who have insulin resistance and pre-diabetes, that do not yet fall into the category of “diabetes”. For diabetics, this would mean their diabetes will worsen by 7%.
Additionally, the study showed that the oral glucose tolerance test AUC only showed a small 0.05% increase. However, if you had no insulin resistance, no pre-diabetes, and no diabetes, you did not have this increase. It only affects those with pre-existing insulin resistance.
Read the study at:
https://www.ahajournals.org/doi/10.1161/ATVBAHA.121.316159
Diabetes Is Genetic
It’s important to understand that type 2 diabetes is a genetic disorder. You cannot give yourself diabetes. Statins can’t alter your genes and give you diabetes. However, if you are already diabetic, you may need slightly more diabetes medications, or have a slight bump in your blood sugar.
There are 17 different alleles that impart insulin resistance, or type 2 diabetes, to humans. Below is a graphic pointing out the various genes and alleles that are involved in making someone more or less insulin resistant. You can read an entire article on diabetes genetics on my blog.

Statins aren’t going to give anyone new diabetes. They may, however, slightly worsen preexisting diabetes. If you are on the border of being “diabetic”, a statin may push you over the edge with that extra 0.1% increase in A1c and that may be enough to initiate diabetes medications.
The article is a fantastic overview of the genetics of diabetes and all the progress we have made in this field:
https://pubmed.ncbi.nlm.nih.gov/18782870/
Other studies on the genetics of type 2 diabetes:
https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.119.316065
https://diabetesjournals.org/care/article/45/3/674/141024/Type-2-Diabetes-Partitioned-Polygenic-Scores
Diabetes, Medications, and Risk For Diabetes
Back to diabetes and statin medications.
You must evaluate the risk to benefit ratio. Diabetics are one of the highest risk populations when it comes to heart disease. Saying that you don’t want to take a statin because you might have a 0.1% increase in your A1c is ridiculous. You will reduce cardiovascular mortality and events rates many times over that 0.1%.
All the guidelines by the American Heart Association, American College of Cardiology, European Atherosclerotic Society, and American Diabetes Association call for a much more aggressive lipid lowering strategy for diabetics because their risk is much higher. They have smaller, atretic arteries, elevated blood sugar, elevated blood pressure, kidney disease, insulin resistance, and dangerously elevated LDL-C. All of these are pounding their arteries and destroying them.
In a study that included over 700,000 participants taking statins, you saw a 7.9% increase in diabetes medication intensification, but no new incidence of diabetes.
Study:
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2784799
A recent study published in The Lancet in March of 2024 looked at 123,940 patients and statin usage over 4.9 years of media follow up. They found that non-diabetics went on to develop diabetes around 10-36% of the time depending on how intense the statin dose was that was being used versus placebo. For example, they found that low dose statin users went on to develop diabetes at a rate of 1.3% per year versus the placebo group which went on to develop diabetes at a rate of 1.2% per year. That’s quite low.
Further, the non-diabetics that went on to develop diabetes were those who had “baseline glycaemic markers that are close to the diagnostic threshold for diabetes”. That’s an exact quote. If your bloodwork demonstrated that you already had insulin resistance and you were near the threshold of being diabetic, then you could be pushed over the edge enough to be considered diabetic.
Study:
https://www.thelancet.com/journals/landia/article/PIIS2213-8587(24)00040-8/fulltext
Is Diet Contributing to Diabetes On Statins?
Another confounding factor to consider is that people are not as strict with their diets once they are placed on medications. They may eat slightly more and gain some weight, which could push their blood tests over the edge into “diabetes range”. Studies try to correct for this, but it’s hard with living breathing people that are living their lives out in the public. With a metabolic ward study, it would be easier to control for this.
Other Diabetogenic Medications
Many other medications that we take daily are also slightly diabetogenic and don’t seem to receive as much bad publicity as statins. Medications like beta blockers (metoprolol), hydrochlorothiazide, steroids, and some antipsychotics are also slightly diabetogenic (cause or worsen diabetes). You must weigh the risks versus benefits individually, and for most diabetics, statins are required for good quality of life and longevity. This must be an informed decision by the patient. We do that with everything, not just medications.
Did You Like This Article?
This post is a chapter from my new Cholesterol Book. If you want updates on when that book will be ready for purchase, click on my updates link and sign up to receive updates:
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















