

Inflammation Does Not Cause Heart Disease
Jan 27, 2025
Does Inflammation Cause Heart Disease?
In the 1970s, there was this theory that cholesterol only came to the arteries to patch up damaged artery walls. The theory was that you must have damage first, then the cholesterol would come in to fix it. This theory also extended to inflammation. That if arteries were inflamed and injured, then cholesterol was just the good guy coming in to patch up the damage.
Does Cholesterol Patch Up Damage?
We had thought that it was like plastering a hole in the wall. Let’s say your kids are wrestling, someone’s elbow puts a hole in the drywall, you get some plaster to fill in the hole. That was our theory.
This was called the “response to injury” hypothesis. Scientists are brilliant and always want to know the truth and want to advance medical knowledge. They also want to advance science and advance our understanding. They also want to win the Nobel Prize in medicine.
Studies from the 1970s and 80s on the response to injury hypothesis:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2279533/
https://www.nejm.org/doi/full/10.1056/NEJM198602203140806
https://www.annualreviews.org/doi/10.1146/annurev.me.30.020179.000245
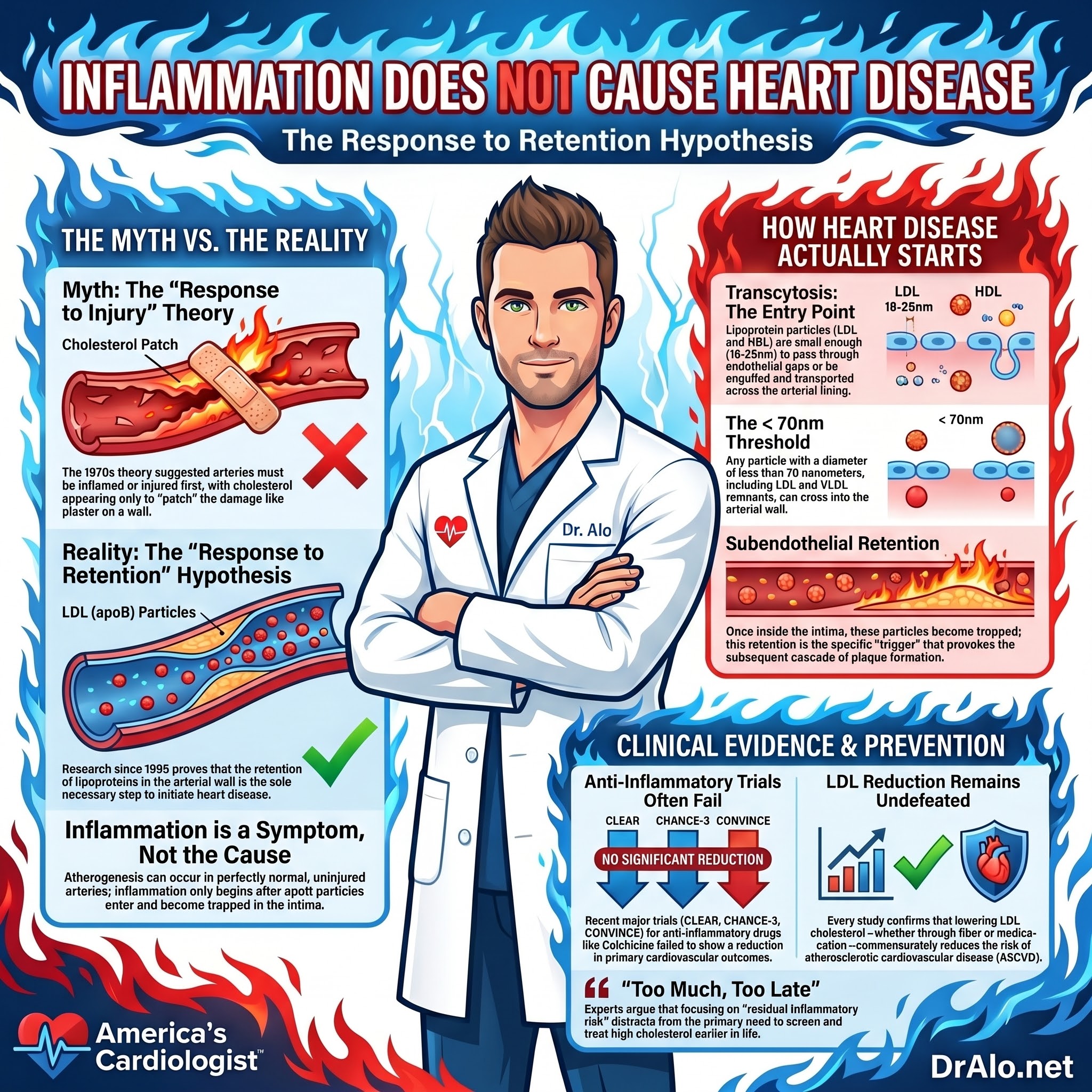
Infographic Summary:
How Arteries Actually Heal?
This has been studied by Williams and Tabas as well and they have published extensively on this topic.
They have found that anything that lower LDL cholesterol, lower atherosclerosis. It does not matter what it is. It can be increased fiber intake, or any new novel medication. Anything that lowers LDL, lowers ASCVD. This remains undefeated. Not only that, but the risk goes down commiserate with the LDL lowering effect. If you lower LDL slightly, you get some reduction of risk. If you lower LDL a lot, you get "a lot" of risk reduction.
Studies previously on anti inflammatory meds have failed to show reduction in CVD risk. There are a multitude of "anti inflammatory" meds that have been tested, and none have lowered CVD risk.
Study:
https://www.ahajournals.org/doi/full/10.1161/CIRCRESAHA.115.307609
So, does inflammation cause atherosclerotic heart disease?
We have spent a considerable amount of time, effort, and money trying to prove whether or not this was true. So that we can better understand the process of atherogenesis.
It was confusing, because many people had no injury and no inflammation, but were still having atherosclerotic heart disease. Atherogenesis can occur in normal arteries without the presence of pre-existing inflammation or arterial lining (endothelial) damage.
After decades of research, it turns out the only necessary component of heart disease, the only thin necessary is a high concentration of LDL-c or low density lipoproteins. This has stood undefeated. Whether you had inflammation or not, if your LDL cholesterol (or apoB) was elevated, you had atherosclerosis.

Drugs Trials And Inflammation
Drugs that lowered damage, like anti-hypertensives, anti-diabetic medications, anti-inflammatory medications had no effect and no benefit. Whereas medications that lowered cholesterol were the only things that worked. We needed answers.
Finally, by 1995, we had our answer.
In 1995, thanks to Williams and Tabas, we got a lot smarter when they published their response to retention hypothesis.
Full read:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2924812
Researchers had spent the last two decades trying to understand what the initiating step in atherosclerosis was. What step was necessary, and without which, there would be no atherosclerosis? Also, they wanted to understand what other factors contributed, but were not sufficient, to cause atherosclerosis.
In their own words…
“Many processes have been implicated in early atherogenesis. These include endothelial denudation, injury, or activation, including shear stress–related events; local adherence of platelets; lipoprotein oxidation; lipoprotein aggregation; macrophage chemotaxis and foam cell formation; and smooth muscle cell alterations. Which process, if any, could be regarded as the key event in early atherogenesis, i.e., absolutely required, yet also sufficient as the sole pathological stimulus in an otherwise normal artery to provoke a cascade of events leading to lesion formation? The work of many investigators, which we summarize here, strongly supports subendothelial retention of atherogenic lipoproteins as the central pathogenic process in atherogenisis. Our thesis is that other contributory processes are either not individually necessary or are not sufficient. Most often, they are merely normal, expected responses of otherwise-healthy tissue to the presence of retained lipoproteins”. [emphasis added]
Read it at:
https://www.ahajournals.org/doi/10.1161/01.ATV.15.5.551
Lipoprotein Retention Is The Only Necessary Step
This is a very high standard and would be quite an achievement. If we could find this single step or single process, we could then target this to eradicate heart disease forever. I believe we have the answer and can do this!
The researchers found that you need a fully intact, uninjured endothelium in order for atherosclerosis to occur. That if you had an injured endothelium (denuded), it would just scar or scab over and heal.
But no atherogenesis would take place.
They also discovered that LDL and HDL particles are always crossing the endothelium and going back and forth. These lipoprotein particles, whose diameter is 8-13 nanometers (nm) for HDL particles and 18-25nm for LDL particles, can pass through endothelial gaps. They can just as easily, freely diffuse, or via receptor internalization, pass through the endothelium. In fact, any particle with a diameter < 70nm can pass through the endothelium which is why chylomicron remnants and VLDL remnants can pass through.
Lipoproteins are tiny and can pass through gap junctions between cells. Gap junctions are small gaps between cells that allow for passive diffusion of electrolytes, molecules, particles, and other small items.
All of these processes fall under the umbrella of transcytosis. Another way that lipoproteins transverse across the cells to enter the intima is through the process depicted below. The outer layer of the cell, the part facing the bloodstream, engulfs an LDL particle and it travels through to the other side.
Take a look at the Supplemental Guide for the images from this section. Or check them out in the article linked below.
From:
https://www.mdpi.com/2073-4409/11/19/3044
On the left is one method of transcytosis in a coronary artery endothelial cell that allows the LDL particles to pass all the way through to the other side. The LDL particle is engulfed and transported over into the intima. The rest of the story happens in the intima. Notice on the right side of the above image is another endothelial cell that did not allow the LDL particles to cross, but instead degraded them internally.
Once apoB particles enter the intima, they cause inflammation. This has been studied extensively and confirmed in multiple studies.
Inflammation is caused by apoB particles in the intima, not the other way around:
https://www.nejm.org/doi/full/10.1056/NEJMra043430
https://pubmed.ncbi.nlm.nih.gov/10922059/
https://pubmed.ncbi.nlm.nih.gov/15809308/
Preventing Heart Disease
If you want to prevent heart disease, the message is clear, get the LDL as low as possible for as long as possible. It's never too late.

Future Medications and Targets
There are novel agents in medications like canikinumab and colchicine that target the inflammation that is present once ASCVD has been established. These are still under investitation. They are not used in primary prevention. These will be for people with established ASCVD.
Study:
https://pubmed.ncbi.nlm.nih.gov/29557210/
The Colchicine Synergy Trial showed no benefit. Colchicine is an anti inflammatory medication.
Study:
https://www.acc.org/Latest-in-Cardiology/Clinical-Trials/2024/10/25/04/34/clear-synergy
Two other studies on Colchicine showed benefit in the Acute MI setting, those having an active heart attack as well as those with established ASCVD.
Studies:
https://www.nejm.org/doi/full/10.1056/NEJMoa1912388
https://www.nejm.org/doi/full/10.1056/NEJMoa2021372
Another recent review article reviewed all of the current evidence on inflammation and heart disease and concluded that it does not play a role in heart disease.
They concluded, "The burden of proof that the Big Idea of inflammation in atherosclerosis has clinical value remains the responsibility of its advocates. This responsibility requires convincing trial data but still seems largely unmet. Unfortunately, the focus on inflammation as the source of residual ASCVD event risk has distracted us from the need to screen and treat earlier".
KEY POINTS From The Review:
- Recent clinical trials challenge the efficacy of colchicine, the sole anti-inflammatory agent currently approved for treatment of atherosclerotic cardiovascular disease.
- Residual ASCVD event risk after optimal management of standard modifiable risk factors may arise primarily from treating too late, rather than from residual inflammatory risk.
- Lipid-lowering therapy in early atherosclerosis, possibly combined with novel add-on agents to accelerate resolution of maladaptive inflammation, may show promise.
- A revolution in noninvasive imaging of the arterial wall is changing screening, diagnosis, and treatment of atherosclerosis, including early and possibly reversable disease.
- The burden of proof that the Big Idea of inflammation in atherosclerosis has clinical value remains the responsibility of its advocates.
They continued...
In 2023, regulatory approval of colchicine produced a great deal of excitement. An old medicine for other disorders, it was a new first-in-class agent in atherosclerosis, and had clinical trial data behind it. Moreover, colchicine seemed to address a major problem, namely, residual ASCVD event risk, which is the persistence of atherosclerotic heart attacks, strokes, and new-onset symptomatic peripheral artery disease in patients after optimal management of their conventional modifiable risk factors for ASCVD events.
But 2024 turned into a rough year for colchicine. Two randomized controlled clinical trials of colchicine in patients with recent stroke, CHANCE-3 and CONVINCE, failed to show benefit [34▪▪,35▪▪]. More troubling, the largest clinical trial to date of colchicine in myocardial infarction (MI), CLEAR (OASIS 9), which had a similar design to the earlier COLCOT trial, failed to show any benefit in the primary outcome, nor across components of the primary outcome. The result is reminiscent of the tiny treatment effect of colchicine in the Dutch patients in the LoDoCo2 trial, as opposed to the robust effect in the Australian patients. In the CLEAR trial, colchicine lowered serum levels of CRP, indicating an anti-inflammatory effect, but ‘The only signal from this trial was an increased risk of diarrhea,’ said the first author, Dr Sanjit Jolly, in an interview just after the first public presentation of the results [38▪]. In the discussion section of the full report, the authors argued, ‘In our trial, 649 first primary-outcome events occurred; an analysis of previous trials showed that those with more than 600 outcome events rarely produced spurious results disproven by subsequent trials’ (pp. 8–9 of the ePub. Dr Jolly also related that he had put his own father on colchicine after an MI, but immediately discontinued the drug as soon as the CLEAR trial was unblinded.
Anti-inflammatory agents proposed for atherosclerosis have at least two major problems. First, we need our immune systems, in contrast to LDL and other apolipoprotein-B (apoB)-containing lipoproteins, which we need in only miniscule amounts. Second, anti-inflammatory therapies, like lipid-lowering therapies, are studied almost entirely in patients who already have advanced, end-stage arterial disease. I have called this approach ‘too much, too late’. Many other authors have also objected to waiting so long to initiate antiatherosclerotic interventions.
Still Have Questions? Stop Googling and Ask Dr. Alo.
You’ve read the science, but applying it to your own life can be confusing. I created the Dr. Alo VIP Private Community to be a sanctuary away from social media noise.
Inside, you get:
-
Direct Access: I answer member questions personally 24/7/365.
-
Weekly Live Streams: Deep dives into your specific health challenges.
-
Vetted Science: No fads, just evidence-based cardiology and weight loss.
Don't leave your heart health to chance. Get the guidance you deserve. All this for less than 0.01% the cost of health insurance! You can cancel at anytime!
[👉 Join the Dr. Alo VIP Community Today]
Cardiology & Obesity Medicine


















